
Comparison of Long-Term Outcomes and Associated Factors between Younger and Older Rural Ischemic Stroke Patients

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Cohort Definition and Outcome Measures
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics and Stroke Risk Factors
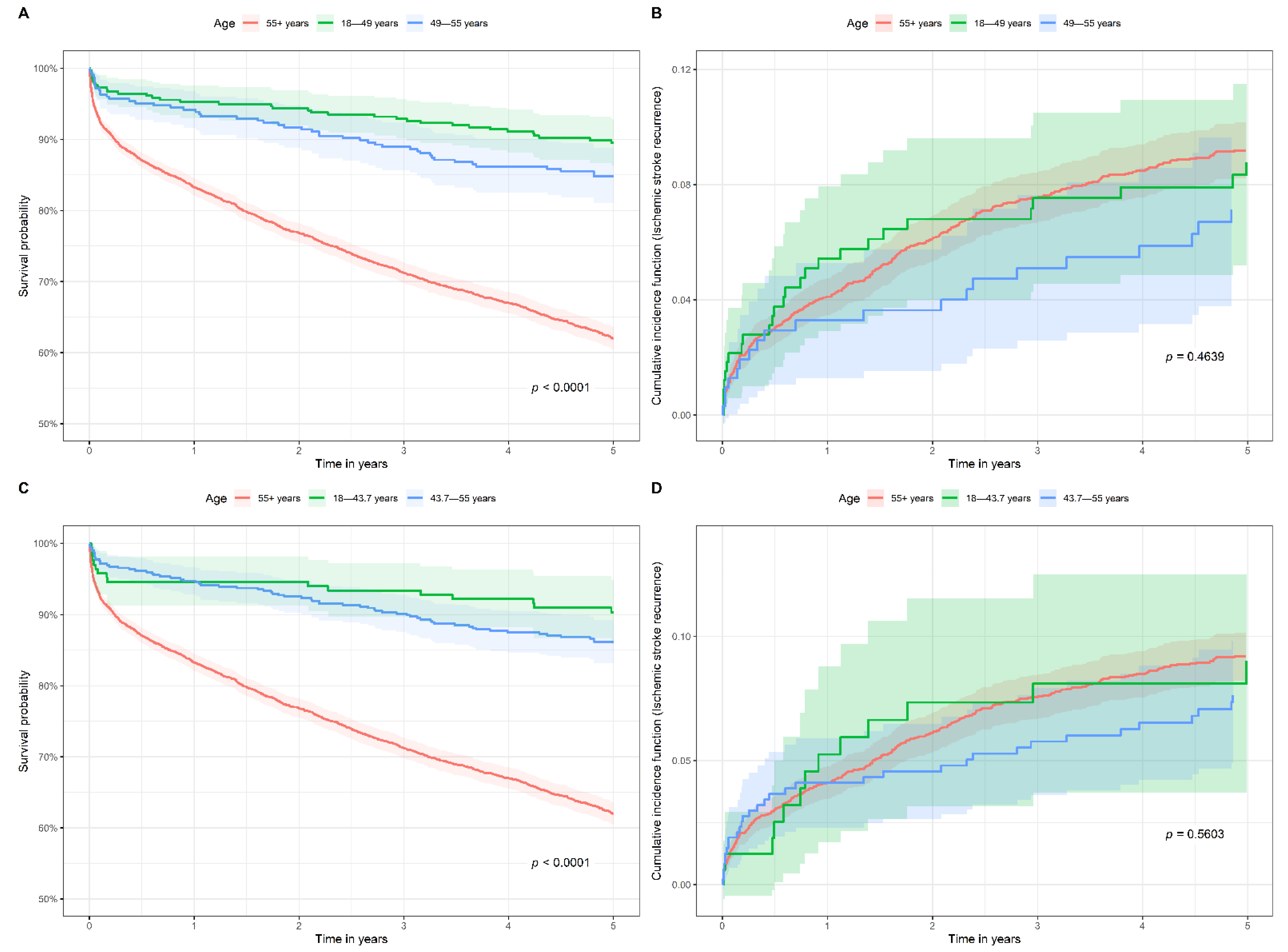
3.2. All-Cause Mortality within 5 Years of Index Stroke in Young Stroke Patients
3.3. Ischemic Stroke Recurrence within Five Years of Index Stroke in Young Stroke Patients
3.4. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maaijwee, N.A.M.M.; Rutten-Jacobs, L.C.A.; Schaapsmeerders, P.; Van Dijk, E.J.; De Leeuw, F.E. Ischaemic stroke in young adults: Risk factors and long-term consequences. In Nature Reviews Neurology; Nature Publishing Group: Berlin, Germany, 2014; pp. 315–325. [Google Scholar]
- Putaala, J. Ischemic stroke in the young: Current perspectives on incidence, risk factors, and cardiovascular prognosis. Eur. Stroke J. 2016, 1, 28–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, M.G.; Tong, X.; Bowman, B.A. Prevalence of cardiovascular risk factors and strokes in younger adults. JAMA Neurol. 2017, 74, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Yahya, T.; Jilani, M.H.; Khan, S.U.; Mszar, R.; Hassan, S.Z.; Blaha, M.J.; Blankstein, R.; Virani, S.S.; Johansen, M.C.; Vahidy, F.; et al. Stroke in young adults: Current trends, opportunities for prevention and pathways forward. Am. J. Prev. Cardiol. 2020, 3, 100085. [Google Scholar] [CrossRef] [PubMed]
- Putaala, J.; Curtze, S.; Hiltunen, S.; Tolppanen, H.; Kaste, M.; Tatlisumak, T. Causes of death and predictors of 5-year mortality in young adults after first-ever ischemic stroke: The Helsinki young stroke registry. Stroke 2009, 40, 2698–2703. [Google Scholar] [CrossRef] [PubMed]
- Waje-Andreassen, U.; Thomassen, L.; Jusufovic, M.; Power, K.N.; Eide, G.E.; Vedeler, C.A.; Naess, H. Ischaemic stroke at a young age is a serious event—Final results of a population-based long-term follow-up in Western Norway. Eur. J. Neurol. 2013, 20, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Rutten-Jacobs, L.C.; Arntz, R.M.; Maaijwee, N.A.; Schoonderwaldt, H.C.; Dorresteijn, L.D.; van Dijk, E.J.; de Leeuw, F.E. Long-term mortality after stroke among adults aged 18 to 50 years. JAMA J. Am. Med. Assoc. 2013, 309, 1136–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varona, J.F.; Bermejo, F.; Guerra, J.M.; Molina, J.A. Long-term prognosis of ischemic stroke in young adults: Study of 272 cases. J. Neurol. 2004, 251, 1507–1514. [Google Scholar] [CrossRef]
- Smajlović, D. Strokes in young adults: Epidemiology and prevention. Vasc. Health Risk Manag. 2015, 11, 157. [Google Scholar] [CrossRef] [Green Version]
- Béjot, Y.; Daubail, B.; Jacquin, A.; Durier, J.; Osseby, G.V.; Rouaud, O.; Giroud, M. Trends in the incidence of ischaemic stroke in young adults between 1985 and 2011: The Dijon Stroke Registry. J. Neurol. Neurosurg. Psychiatry 2014, 85, 509–513. [Google Scholar] [CrossRef] [Green Version]
- Cabral, N.L.; Freire, A.T.; Conforto, A.B.; Dos Santos, N.; Reis, F.I.; Nagel, V.; Guesser, V.V.; Safanelli, J.; Longo, A.L. Increase of stroke incidence in young adults in a middle-income country a 10-year population-based study. Stroke 2017, 48, 2925–2930. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan Jr, P.W.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: Executive Summary. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, D.; Khan, A.; Shahjouei, S.; Gupta, M.; Lambert, C.; Avula, V.; Schirmer, C.M.; Holland, N.; Griessenauer, C.J.; Azarpazhooh, M.R.; et al. Trends in ischemic stroke outcomes in a rural population in the United States. J. Neurol. Sci. 2021, 422, 117339. [Google Scholar] [CrossRef] [PubMed]
- Lambert, C.; Chaudhary, D.; Olulana, O.; Shahjouei, S.; Avula, V.; Li, J.; Abedi, V.; Zand, R. Sex disparity in long-term stroke recurrence and mortality in a rural population in the United States. Ther. Adv. Neurol. Disord. 2020, 13, 175628642097189. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, D.; Khan, A.; Gupta, M.; Hu, Y.; Li, J.; Abedi, V.; Zand, R. Obesity and mortality after the first ischemic stroke: Is obesity paradox real? PLoS ONE 2021, 16, e0246877. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.B.; Klein, J.P.; Moeschberger, M.L. Survival Analysis Techniques for Censored and Truncated Data, 2nd ed.; Springer: New York, NY, USA, 1998; Volume 40, p. 159. [Google Scholar]
- Austin, P.C.; Lee, D.S.; Fine, J.P. Introduction to the Analysis of Survival Data in the Presence of Competing Risks. Circulation 2016, 133, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Varona, J.F. Long-term prognosis of ischemic stroke in young adults. Stroke Res. Treat. 2011, 2011, 879817. [Google Scholar] [CrossRef] [Green Version]
- Edwards, J.D.; Kapral, M.K.; Lindsay, M.P.; Fang, J.; Swartz, R.H. Young Stroke Survivors With No Early Recurrence at High Long-Term Risk of Adverse Outcomes. J. Am. Heart Assoc. 2019, 8, e010370. [Google Scholar] [CrossRef] [Green Version]
- Putaala, J.; Metso, A.J.; Metso, T.M.; Konkola, N.; Kraemer, Y.; Haapaniemi, E.; Kaste, M.; Tatlisumak, T. Analysis of 1008 consecutive patients aged 15 to 49 with first-ever ischemic stroke the Helsinki young stroke registry. Stroke 2009, 40, 1195–1203. [Google Scholar] [CrossRef] [Green Version]
- Marini, C.; Totaro, R.; Carolei, A. Long-Term Prognosis of Cerebral Ischemia in Young Adults. Stroke 1999, 30, 2320–2325. [Google Scholar] [CrossRef] [Green Version]
- Putaala, J.; Yesilot, N.; Waje-Andreassen, U.; Pitkäniemi, J.; Vassilopoulou, S.; Nardi, K.; Odier, C.; Hofgart, G.; Engelter, S.; Burow, A.; et al. Demographic and geographic vascular risk factor differences in european young adults with ischemic stroke: The 15 cities young stroke study. Stroke 2012, 43, 2624–2630. [Google Scholar] [CrossRef] [Green Version]
- Leys, D.; Bandu, L.; Henon, H.; Lucas, C.; Mounier-Vehier, F.; Rondepierre, P.; Godefroy, O. Clinical outcome in 287 consecutive young adults (15 to 45 years) with ischemic stroke. Neurology 2002, 59, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaap Kappelle, L.; Adams, H.P.; Heffner, M.L.; Torner, J.C.; Gomez, F. Prognosis of Young Adults With Ischemic Stroke A Long-term Follow-up Study Assessing Recurrent Vascular Events and Functional Outcome in the Iowa Registry of Stroke in Young Adults. Stroke 1994, 25, 1360–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekker, M.S.; Verhoeven, J.I.; Vaartjes, I.; Van Nieuwenhuizen, K.M.; Klijn, C.J.M.; De Leeuw, F.E. Stroke incidence in young adults according to age, subtype, sex, and time trends. Neurology 2019, 92, e2444–e2454. [Google Scholar] [CrossRef] [PubMed]
- Rutten-Jacobs, L.C.; Maaijwee, N.A.; Arntz, R.M.; Schoonderwaldt, H.C.; Dorresteijn, L.D.; van der Vlugt, M.J.; van Dijk, E.J.; de Leeuw, F.E. Long-term risk of recurrent vascular events after young stroke: The FUTURE study. Ann. Neurol. 2013, 74, 592–601. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | 18–55 Age Group | >55 Age Group | p | |
|---|---|---|---|---|
| Number of patients, n | 4459 | 664 | 3795 | |
| Sex: Male, n (%) | 2305 (51.7) | 394 (59.3) | 1911 (50.4) | <0.001 |
| Age at index stroke in years, median [IQR] | 71.5 [60.7, 80.8] | 49.0 [43.7, 52.4] | 74.4 [65.8, 82.0] | - |
| Hypertension, n (%) | 3169 (71.1) | 346 (52.1) | 2823 (74.4) | <0.001 |
| Atrial fibrillation, n (%) | 814 (18.3) | 14 (2.1) | 800 (21.1) | <0.001 |
| Dyslipidemia, n (%) | 2555 (57.3) | 283 (42.6) | 2272 (59.9) | <0.001 |
| Diabetes, n (%) | 1338 (30.0) | 164 (24.7) | 1174 (30.9) | 0.001 |
| Congestive heart failure, n (%) | 519 (11.6) | 23 (3.5) | 496 (13.1) | <0.001 |
| Myocardial infarction, n (%) | 473 (10.6) | 41 (6.2) | 432 (11.4) | <0.001 |
| Peripheral vascular disease, n (%) | 685 (15.4) | 48 (7.2) | 637 (16.8) | <0.001 |
| Hypercoagulable state, n (%) | 59 (1.3) | 22 (3.3) | 37 (1.0) | <0.001 |
| Chronic kidney disease, n (%) | 604 (13.5) | 36 (5.4) | 568 (15.0) | <0.001 |
| Neoplasm, n (%) | 684 (15.3) | 23 (3.5) | 661 (17.4) | <0.001 |
| Rheumatic diseases, n (%) | 165 (3.7) | 12 (1.8) | 153 (4.0) | 0.007 |
| Patent foramen ovale, n (%) | 384 (8.6) | 128 (19.3) | 256 (6.7) | <0.001 |
| Smoking status | <0.001 | |||
| Current smoker, n (%) | 563 (12.6) | 170 (25.6) | 393 (10.4) | |
| Former smoker, n (%) | 956 (21.4) | 72 (10.8) | 884 (23.3) | |
| Never smoker, n (%) | 1275 (28.6) | 136 (20.5) | 1139 (30.0) | |
| Unknown, n (%) | 1665 (37.3) | 286 (43.1) | 1379 (36.3) | |
| NIHSS *, median [IQR] | 4.0 [2.0, 7.0] | 3.0 [1.0, 6.0] | 4.0 [2.0, 7.0] | 0.015 |
| All-Cause Mortality at 5 Years in the 18–55 Age Group | Ischemic Stroke Recurrence at 5 Years in the 18–55 Age Group | |||||
|---|---|---|---|---|---|---|
| Alive | Deceased | p | No Recurrence | Recurrence | p | |
| Number of patients, n | 580 | 84 | 338 | 46 | ||
| Sex: Male, n (%) | 341 (58.8) | 53 (63.1) | 0.528 | 193 (57.1) | 24 (52.2) | 0.636 |
| Age at index stroke in years, median [IQR] | 48.7 [43.5, 52.4] | 49.9 [45.9, 52.3] | 0.082 | 48.8 [43.4, 52.3] | 47.7 [43.5, 51.8] | 0.627 |
| Hypertension, n (%) | 293 (50.5) | 53 (63.1) | 0.041 | 164 (48.5) | 21 (45.7) | 0.835 |
| Atrial fibrillation, n (%) | 11 (1.9) | 3 (3.6) | 0.403 | 5 (1.5) | 0 (0.0) | 1.000 |
| Dyslipidemia, n (%) | 244 (42.1) | 39 (46.4) | 0.524 | 143 (42.3) | 23 (50.0) | 0.407 |
| Diabetes, n (%) | 129 (22.2) | 35 (41.7) | <0.001 | 67 (19.8) | 15 (32.6) | 0.073 |
| Congestive heart failure, n (%) | 15 (2.6) | 8 (9.5) | 0.003 | 8 (2.4) | 4 (8.7) | 0.043 |
| Myocardial infarction, n (%) | 30 (5.2) | 11 (13.1) | 0.010 | 17 (5.0) | 2 (4.3) | 1.000 |
| Peripheral vascular disease, n (%) | 33 (5.7) | 15 (17.9) | <0.001 | 22 (6.5) | 5 (10.9) | 0.349 |
| Hypercoagulable state, n (%) | 18 (3.1) | 4 (4.8) | 0.508 | 10 (3.0) | 2 (4.3) | 0.644 |
| Chronic kidney disease, n (%) | 20 (3.4) | 16 (19.0) | <0.001 | 13 (3.8) | 3 (6.5) | 0.422 |
| Neoplasm, n (%) | 18 (3.1) | 5 (6.0) | 0.196 | 10 (3.0) | 3 (6.5) | 0.195 |
| Rheumatic diseases, n (%) | 10 (1.7) | 2 (2.4) | 0.656 | 6 (1.8) | 1 (2.2) | 0.594 |
| Patent foramen ovale, n (%) | 120 (20.7) | 8 (9.5) | 0.023 | 73 (21.6) | 11 (23.9) | 0.868 |
| Smoking status | 0.146 | 0.004 | ||||
| Current smoker, n (%) | 145 (25.0) | 25 (29.8) | 92 (27.2) | 16 (34.8) | ||
| Former smoker, n (%) | 58 (10.0) | 14 (16.7) | 37 (10.9) | 6 (13.0) | ||
| Never smoker, n (%) | 123 (21.2) | 13 (15.5) | 69 (20.4) | 17 (37.0) | ||
| Unknown, n (%) | 254 (43.8) | 32 (38.1) | 140 (41.4) | 7 (15.2) | ||
| NIHSS, median [IQR] | 3.0 [1.0, 6.0] | 2.0 [1.0, 3.5] | 0.666 | 4.0 [1.5, 7.0] | 3.0 [2.0, 3.8] | 0.654 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhary, D.; Anyaehie, M.; Demiraj, F.; Bavishi, S.; Shahjouei, S.; Li, J.; Abedi, V.; Zand, R. Comparison of Long-Term Outcomes and Associated Factors between Younger and Older Rural Ischemic Stroke Patients. J. Clin. Med. 2022, 11, 1430. https://doi.org/10.3390/jcm11051430
Chaudhary D, Anyaehie M, Demiraj F, Bavishi S, Shahjouei S, Li J, Abedi V, Zand R. Comparison of Long-Term Outcomes and Associated Factors between Younger and Older Rural Ischemic Stroke Patients. Journal of Clinical Medicine. 2022; 11(5):1430. https://doi.org/10.3390/jcm11051430
Chicago/Turabian StyleChaudhary, Durgesh, Michelle Anyaehie, Francis Demiraj, Shreya Bavishi, Shima Shahjouei, Jiang Li, Vida Abedi, and Ramin Zand. 2022. "Comparison of Long-Term Outcomes and Associated Factors between Younger and Older Rural Ischemic Stroke Patients" Journal of Clinical Medicine 11, no. 5: 1430. https://doi.org/10.3390/jcm11051430